

Abstract
The last two authors contributed equally
Elevated soluble Stimulation-2 (sST2), the decoy IL-33 receptor, in plasma/serum post-HSCT is a biomarker for death due to GvHD. ST2 is the product of IL1RL1 (2q12.1) and this ~.5Mb region contains >300 single nucleotide polymorphisms (SNPs) significantly associated (P<5x10-8) with plasma levels of sST2 in healthy participants from the Framingham Heart Study (FHS). Many of these SNPs are genome-wide associated with infection-related phenotypes, including asthma, Crohn's disease, ulcerative colitis and celiac disease. Given these relationships, we analyzed the association of ST2 SNPs with death due to GvHD or infection within one year after HLA-matched unrelated donor HCT for AML or MDS to identify functional SNPs that could potentially aid in donor selection.
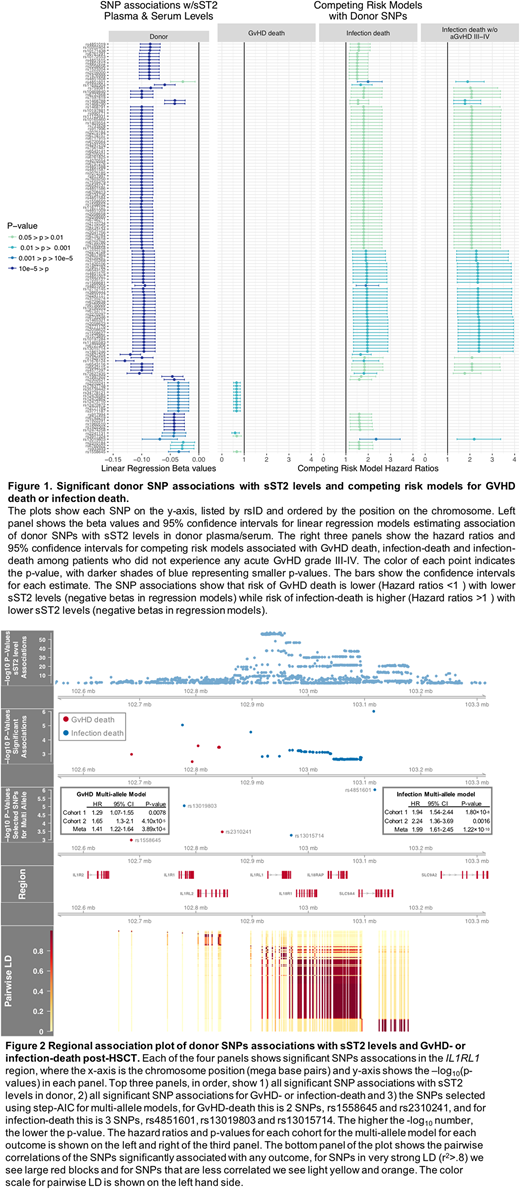
We measured plasma/serum sST2 levels in pre-HCT samples in a subset of AML and MDS patients (n=759) and their donors (n=757) from DISCOVeRY-BMT, a GWAS of >3,000 recipient-unrelated donor pairs reported to the CIBMTR between 2000-2011. After quality control (info>.8, MAF>.005), 3613 SNPs in the IL1RL1 region were tested for association with sST2 levels; 1541 donor SNPs associated with sST2 levels (P<.05), which validated 99% of the FHS sST2 SNP associations. To assess the contribution of these donor variants to post-HCT survival, we constructed competing risk models with clinical variables using stepwise Akaike Information Criterion (AIC), then tested each of the 1541 donor SNPs for association with each outcome in the two DISCOVeRY-BMT cohorts. Causes of death were previously adjudicated by a multi-member panel. Meta-analyses of the two cohorts identified 13 GvHD-death associated SNPs and 118 infection-death associated SNPs. Sensitivity analyses show 91/118 SNPs are still significant after excluding patients with a history of acute GvHD grade III-IV (Figure 1). When taking correlations into account, we found 10 and three independent SNPs (R2<.6) associate with death due to infection and GvHD, respectively. There were no overlapping SNP associations between GvHD-death or infection-death (Figure 1). For GvHD-death associated SNPs, alleles associated with higher sST2 levels associate with increased risk for GvHD-death, while for infection-death SNPs, alleles associated with higher sST2 levels reduced risk of infection-death.
AIC multivariable models for GvHD-death included AML diagnosis, recipient obesity (>30 mg/kg2), peripheral blood cell source, donor age, rs1558645 (Pmeta=.001), and rs2310241(Pmeta=.0003), for which the risk alleles at each SNP increased risk of GvHD death ~1.5 fold. The model for infection-death included advanced disease at HCT, recipient/donor CMV status, peripheral blood cell source, rs13019803 (Pmeta=1.1 x 10-6), rs13015714 (Pmeta=5 x 10-4) and rs4851601 (Pmeta=2 x 10-6), with risk alleles at each SNP increasing risk of infection-death ~2-fold. To capture the total contribution of these donor variants to each outcome we created multi-allele models for GvHD-death (0-4 alleles) and infection-death (0-6 alleles).The multi-allele GvHD models showed a 1.5 fold increased risk of GvHD-death with each additional allele (Pmeta=3.4 x 10-6 ) (Figure 2). Individuals whose donors are homozygous for both risk alleles at each SNP have a ~3 fold, and ~2 fold higher risk of dying of GvHD versus those with zero, and 1-2 risk allele(s), respectively. The multi-allele infection models (0-6 alleles) show a ~2 fold increased risk of infection-death (Pmeta= 1.22 x 10-10) with each risk allele (Figure 2).
sST2 is one of the most reproducible GvHD biomarkers to date. As hypothesized, specific alleles correlated with high sST2 levels in donors and with GvHD-death. Our novel finding is that some ST2 alleles associated with low sST2 levels correlated with infection-death. These results are not without precedent, for example the low-sST2 associated allele in rs13019803 (T) associates with higher mortality in the CHARGE consortium. The risk allele in rs13015714 (T) is significantly associated with lower IL1RL1 and IL18R1 (P= 5 x 10-10) gene expression in lung tissue, indicating biochemical functions for these SNPs. Importantly the non-risk allele in all 5 variants are common (>20%) across races and ethnicities, which means there is an opportunity to select donors without combinations of these variants and perhaps without the requirement of measuring the protein level pre-transplant.
McCarthy:Karyopharm: Consultancy, Honoraria; Takeda: Consultancy, Honoraria; Bristol Myers Squibb: Consultancy, Honoraria; Celgene: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria. Lee:Kadmon: Research Funding; Amgen: Consultancy, Research Funding; Mallinckrodt: Honoraria; Incyte: Consultancy; Pfizer: Consultancy; Onyx: Research Funding; Takeda: Research Funding. Paczesny:Viracor IBT Laboratories: Patents & Royalties.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal